We often talk about the deleterious short-term and long-term side effects when it comes to drugs, i.e. how the QUALITY of our lives are affected.
But rarely do we stop and think about how these drugs affect our longevity — the QUANTITY of years we have to inhabit our meat suits.
Two classes of drugs I’ve prolifically attacked in recent times are estrogen inhibitors and DHT inhibitors.
And not without good reason… I’ve either spent years using them and/or know people who have and had to watch them suffer in agony and silence.
Showing how these drugs ruin men’s health is the easy part. Proving they shave years of optimized life off our limited time on this Earth is another endeavor altogether.
Today, however, marks the first time I have conclusive evidence of both types of drugs shortening human lifespan.
MAJOR credit has to be given to Dr. Scott Howell for compiling all of the research and the main talking points featured in his article. Not only does his write-up back up what I’ve known and said for the past decade, but also adds in new scientifically backed information I didn’t even know about.
At the end of this article I will tell you how to reach out to him for his guidance in harm reduction. If you do not work with him for whatever reason, I implore you to share this article with your friends and family at a bare minimum. This type of information can and will SAVE LIVES. But only if it’s placed into the right hands!
PART 1: DHT Inhibiting Drugs

Before you start reading this section, you need to get yourself caught up to speed about the 5α-reductase inhibitors (5-ARIs) and why it’s a bad idea to inhibit the conversion of testosterone to dihydrotestosterone (DHT).

(Source)
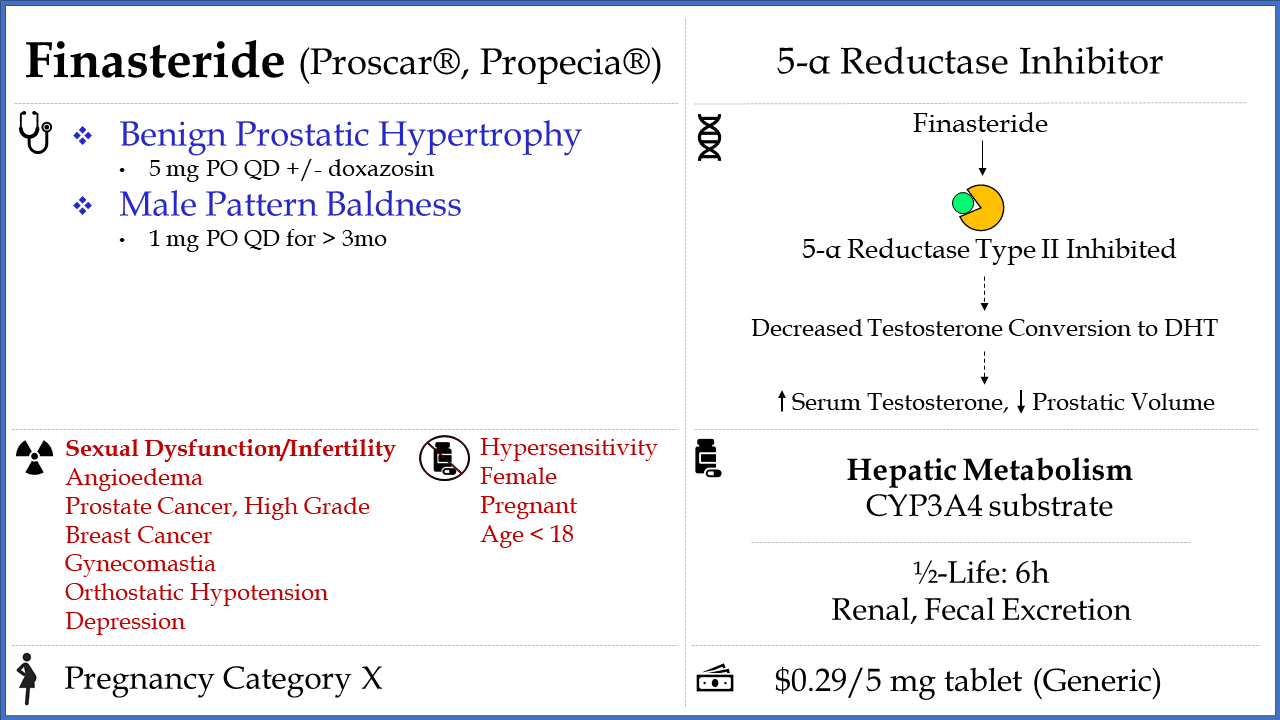
First, read the definitive article I’ve written about why DHT-inhibiting drugs like Finasteride and Dutasteride DO NOT work for hair loss in the way you’ve been led to believe.
You’ll discover why at best they address a secondary cause of hair loss while failing to tackle the root causes, along with a nasty side effect profile that includes increased fat accumulation, gynecomastia, and higher rates of depression.
Second, educate yourself on why DHT-inhibiting drugs can lead to long-term (if not permanent) sexual dysfunction in men EVEN when the drugs are no longer being used.
You might as well play Russian roulette instead of using them.
Some Background Information on the 5-Alpha-Reductase Enzyme
Thanks to a landmark paper published by Faris Azzouni et al. in 2012, we can better understand the importance of this enzyme and all of the major biological functions it is responsible for in the human body.
Our journey starts in the 1950s, where these enzymes were first isolated and their characteristics further studied:
“Steroid-5-reductases (5α-R and 5β-R) were first discovered, purified, and characterized in rat liver homogenates. These early experiments demonstrated that these enzymes were capable of irreversibly reducing the delta 4, 5 bond (double bond between carbons 4 and 5; Δ4,5) of C-19 and C-21 steroids to 5α- and 5β-stereoisomers.”
“…In the 1960s, 5α-reduction was shown to be an irreversible reaction and DHT was found to be a more potent androgen than T in prostate bioassays. The administration of radiolabeled T to rats resulted in a time-dependent accumulation of DHT in the nuclei of ventral prostate cells, which subsequently bound to a specific nuclear (androgen) receptor. These data indicated that 5α-reduction of T is a crucial step in androgen action and focused attention on 5α-R”
As it turns out, we now know that there are THREE subfamilies that make up the entirety of all 5α-R enzymes:
- Subfamily #1: 5α-R1, 5α-R2
- Subfamily #2: 5α-3
- Subfamily #3: The glycoprotein synaptic 2 protein (GPSN2) and glycoprotein synaptic 2-like protein (GPSN2L)
In total, we have 3 isozymes (i.e. proteins that perform the same function) of the 5α-R enzyme and two other proteins that have the capability to act like the 5α-R enzyme.
This is important because the DHT-inhibiting drugs we are all familiar with actually function by targeting different enzymes:
“The conversion of testosterone to dihydrotestosterone is catalyzed by the enzyme 5α-reductase (5AR), which exists in 2 forms: Type 1 and Type 2, both of which are found in the prostate.
Type 1 is produced primarily in liver and skin and is carried to the prostate via the systemic circulation. Type 2 is the major form in the prostate.
Finasteride inhibits Type 2 5AR. Dutasteride inhibits both Type 1 and 2 5AR (dual inhibitor). DHT, dihydrotestosterone.”
Now, as we already know, DHT is responsible for in utero differentiation and growth of the prostate and male external genitalia, and during puberty it is responsible for the growth of facial and body hair between the sexes (alongside penis and scrotum growth in males).
This became evident when we studied male pseudohermaphrodites in the 1970s and their lack of DHT production:
“Guevedoces” (literally, penis at 12) of Dominican Republic are biological males (46XY) with female-appearing external genitalia from birth until puberty; at puberty, they develop a penis, the testes descend, muscles and a male psychosexual orientation develop. Throughout life, the prostate remains small, because the congenital deficiency of 5α-reductase leaves affected individuals with markedly suppressed levels of dihydrotestosterone (DHT).”
“…Scientists in the pharmaceutical industry reasoned that if 5AR could be targeted for inhibition after the external genitalia were fully formed and mature, then a safe drug to shrink the prostate, relieve LUTS [lower urinary tract symptoms], and ameliorate baldness and acne might be developed”
The 5-Alpha-Reductase Enzyme Is Found In Numerous Parts Of The Body Throughout Human Life
Thanks to Azzouni et al.’s compilation of data, they discovered the 5α-R enzymes are expressed throughout the entirety of human development in various tissues.
Developing Fetus:
- 5α-R1 is expressed 5-50x lower in non-genital skin and scalp compared to adult skin
- 5α-R2 has a similar level of expression as adults in the prostate
At Birth:
- 5α-R1 is expressed in the liver, prostate, scalp, and skin
- 5α-R2 expression is reduced in the scalp and skin, but is also expressed in the epididymis, liver, prostate, and seminal vesicles
- 5α-R1 and 5α-R2 expression in the prostate is lifelong
- After two years, 5α-R1 and 5α-R2 expression are undetectable in the scalp and skin until puberty starts
Adulthood:
- 5α-R1 and 5α-R2 expression is different in the following tissues: Brain, epididymis, kidney, liver, ovary, pancreas, prostate, skin (genital and non-genital), testis, seminal vesicles, uterus
- 5α-R1 expression is present in the stomach, whereas 5α-R2 expression can be found in the lungs
- 5α-R1 expression is observed in the brain, intestine, kidney, liver, pancreas, prostate, skin, testis, and uterus
The 5-Alpha-Reductase Enzyme Affects The Production Of NUMEROUS Steroid Metabolites
Many people fail to realize the 5α-R enzyme doesn’t just convert testosterone into DHT.
According to Wikipedia, there are numerous steroid hormone substrates that are reduced by this enzyme:
- Cholestenone → 5α-Cholestanone
- Progesterone → 5α-Dihydroprogesterone
- 3α-Dihydroprogesterone → Allopregnanolone
- 3β-Dihydroprogesterone → Isopregnanolone
- Deoxycorticosterone → 5α-Dihydrodeoxycorticosterone
- Corticosterone → 5α-Dihydrocorticosterone
- Cortisol → 5α-Dihydrocortisol
- Aldosterone → 5α-Dihydroaldosterone
- Androstenedione → 5α-Androstanedione
- Nandrolone → 5α-Dihydronandrolone
What are the major biological functions of these steroid metabolites, and are we fully aware of the possible yet unknown long-term consequences of continuously inhibiting the 5α-R enzyme?
The Downstream Effects Of 5-Alpha-Reductase Enzyme Inhibition
Let’s take a look at what exactly we’re risking when we ignorantly use 5ARIs and assume we’re “only” tackling the problem of hair loss…
Protein N-Glycosylation
From the Azzouni paper:
“Congenital deficiency of 5α-R3 has been linked to a rare, autosomal recessive disorder in which patients are born with mental retardation, cerebellar, and ophthalmologic [eye] defects.
The presumed defect involves the reduction of the terminal double bond of polyprenols to dolichols, an important step in protein N-glycosylation. N-linked protein glycosylation involves the addition of a 14-sugar glycan to select asparagine residues on a nascent protein to facilitate proper folding and trafficking of the protein and occurs in the membranes of endoplasmic reticula”
To really show you why this is important, Dr. Scott Howell chimes in with his own research:
“Protein N-glycosylation is a metabolic process that has been greatly conserved in evolution and in all eukaryotes, N-glycosylation is necessary to initiate and sustain life, i.e. biological viability: the capacity of being alive; capability of living, developing, or reproducing.
The two intrinsic functions of this process involves providing structural components to cells walls and the extracellular matrix, and modifying protein properties to make them more stable and soluble.
The two extrinsic functions of this process involve directing the trafficking of proteins and mediating cell-signaling (i.e. cell-to-cell, cell-to-matrix interactions)”
A Biomarker For Detecting Malignancy
Believe it or not, refusing to tamper with 5α-R enzyme expression can help us identify the presence of cancers at an early stage.
Azzouni’s paper summarizes what has been found in the literature to date:
- Lower levels of 5α-R2 expression and higher levels of 5α-R1 expression in prostate cancer compared to BPH (benign prostate hyperplasia)
- Higher levels of 5α-R3 expression in castration-recurrent prostate cancer and androgen-stimulated prostate cancer
- Higher levels of 5α-R3 expression in breast, lung, thyroid, and testicular cancers
Here’s the real kicker: Remember earlier in the article when I mentioned finasteride and dutasteride only target 5α-R1 and 5α-R2?
It turns out that in a separate paper published by Azzouni, both DHT-inhibiting drugs can also inhibit 5α-R3 activity:
“Finasteride and dutasteride effectively inhibit 5α-R type 3 in vitro, and near-maximal suppression of intraprostatic DHT with dutasteride 3.5–5 mg daily suggest that development of a triple 5ARI may not be necessary.”
Granted, we don’t have enough clinical data in humans to show this effect can be consistently repeated, but it should give any serious cancer researcher great pause.
Decreased Red Blood Cell Production
Dr. Scott Howell’s reading of the Azzouni paper led to three important conclusions about the production of red blood cells:
- Isomers of 5-α-reduced C-19 steroids directly stimulate hematopoietic stem cells to increase red blood cells, a process known as erythropoiesis.
- Isomers of 5-α-reduced C-19 steroids indirectly stimulate erythropoiesis by increasing kidney-produced EPO (erythropoietin hormone), which then acts to stimulate erythroid precursors to mature and transition into mature red cells.
- 5-β-reduced steroids are important for heme synthesis in the liver, which is required for erythropoiesis.
Here’s an overview of why erythropoiesis is important:
“Erythropoiesis is one of the important physiological supply functions of the bone marrow. In healthy adults, about 200×10 red cells are produced per day in the bone marrow and are released into the peripheral blood.
Depending on demand, red cell production can be adjusted and upregulated substantially. A complex network of oxygen sensors, cytokines, such as erythropoietin, and other factors, including regulators of iron metabolism, are involved in the control of steady-state and stress-induced erythropoiesis, thereby ensuring appropriate oxygen supply to the peripheral tissues.
…In the elderly, the bone marrow and other organs undergo aging. As a result, erythropoietin synthesis and red cell production may decline. However, even in very old individuals, red cell production and erythropoietin synthesis are usually adequate to keep hemoglobin levels within a reasonable range unless certain co-morbidities that lead to insufficient production of red cells have been acquired”
And when you impair erythropoiesis, you end up with anemia:
“Red blood cells contain hemoglobin, a protein that enables them to carry oxygen from the lungs and deliver it to all parts of the body. When the number of red blood cells is reduced, the blood cannot carry an adequate supply of oxygen. An inadequate supply of oxygen in the tissues causes the symptoms of anemia.
…Mild anemia often causes fatigue, weakness, and paleness. In addition to these symptoms, more severe anemia may cause faintness, dizziness, increased thirst, sweating, a weak and rapid pulse, and rapid breathing. Severe anemia may cause painful lower leg cramps during exercise, shortness of breath, and chest pain, especially if people already have impaired blood circulation in the legs or certain types of lung or heart disease.”
Compromised Bile Synthesis
Again, we refer back to the Azzouni paper
“Both 5α-R and 5β-R are involved in bile biosynthesis, where they catalyze the conversion of 7α, 12α-dihydroxy-4-cholesten-3-one into 7α,12α-dihydroxy- 5α-cholestan-3-one, and 7α,12α-dihydroxy-5β-cholestan-3-one, respectively.
Only the 5β-isomer has been shown to be biologically active and is used for bile synthesis. The 5α-isomer is inactive and suggested to be an inhibitory step in bile biosynthesis regulation in humans.”
Put simply, 5-αR acts to inhibit bile synthesis while 5-β-reductase is necessary to stimulate bile synthesis.
Here’s why bile synthesis needs to be properly regulated:
“Bile acids are chemical compounds found in the liver that have several roles in the body including promoting the flow and excretion of bile and assisting in the intestinal absorption of fat and fat-soluble vitamins. Bile acids are formed from cholesterol and, therefore, bile acid synthesis serves as the main pathway in breaking down and eliminating cholesterol from the body (cholesterol degradation).
The failure to produce normal or functional bile acids results in the accumulation of abnormal bile acids and other substances that normally would be broken down (intermediary metabolites) within the body. The resulting accumulation of abnormal bile acids, intermediary metabolites and cholesterol in the body can damage certain organ systems”
One thing we know for sure is that diarrhea rears its ugly head when too much bile is produced:
“Bile acid diarrhea (BAD), sometimes also known as bile acid malabsorption or bile salt malabsorption (though this is not always the correct terminology), can result in symptoms such as bowel frequency, urgency, nocturnal defecation, excessive flatulence, abdominal pain and incontinence of stool. This phenomenon was first described in 1967 and was initially known as choleric enteropathy. It has since been classified as primary BAD which is idiopathic and is usually secondary to hepatic overproduction of bile acids due to interruption of the negative feedback loop rather than malabsorption in the ileum.”
… there is no actual malabsorption in primary BAD, unlike that occurring due to terminal ileal disease such as Crohn’s. Rather, there is hepatic overproduction of bile acids due to interruption of the negative feedback loop regulating bile acid synthesis, resulting in a larger than normal proportion of bile acids entering the colon and exerting its effect”
What else could be a downstream consequence of 5-αR inhibition?
Impaired Eye Health
Remember the list of substrates that the 5-αR enzyme acts on?
One of them is cortisol and it gets enzymatically converted into 5α-dihydrocortisol, which Azzouni says “is present in the aqueous humor of the eye, is synthesized in the lens of the eye, and may play a role in the regulation of aqueous humor formation”.
We don’t know much else, but this small human study conducted in 2020 is a preview of what may happen to some unlucky individuals:
“…This retrospective case-control, cross-sectional study included electronic health record data from 31 male patients who showed foveal cavitation on spectral-domain optical coherence tomography imaging from January 1, 2016, to June 30, 2019.
…Among 31 male patients with foveal cavitation, 5-ARI was used [for at least 2 years for treating BPH and/or androgenic alopecia” for 10 of 14 patients (71.4%) with macular abnormalities of unknown origin and for 2 of 17 patients (11.8%) with macular abnormalities of well-known specific origin
“…The findings suggest that macular abnormalities associated with 5-ARI are characterized by cystoid abnormalities and foveal cavitation in male patients, which may progress to outer foveal defect and macular hole. These macular abnormalities associated with a male sex hormone antagonist suggested by this investigation warrant further corroboration”
How are we just NOW figuring out this information!?
Even MORE Sexual Dysfunction
When I discussed the negative effects on sexual performance associated with DHT inhibitor use in both of my published articles I asked you to read earlier, the bulk of the evidence came from a systematic review published in 2011 by Abdulmaged Traish and his colleagues.
And even though that should have been enough to halt the use of drugs like Dutasteride and Finasteride except in special cases, it seems TPTB (the powers that be) just didn’t see enough of a reason to pull them off the market.
I mean why would they, when hair loss is a multi-billion dollar industry?
Nearly a decade later, the evidence continues to point in the same direction.
In 2016, an observational study conducted by Italian scientists of 79 young men who used finasteride for an average of 27 months and had discontinued finasteride use for an average of 44 months found some shocking observations:
“40.5% of participants declared getting and keeping erection very difficult, and 3.8% never achieved; reaching orgasm was declared very difficult by 16.5%, and never achieved by 2.5%.
By the ad hoc questionnaire, the most frequent sexual symptoms referred were loss of penis sensitivity (87.3%), decreased ejaculatory force (82.3%), and low penile temperature (78.5%).
The most frequent non-sexual symptoms were reduced feeling of life pleasure or emotions (anhedonia) (75.9%); lack of mental concentration (72.2%), and loss of muscle tone/mass (51.9%).”
In a 2021 article examining various therapies causing male infertility, the link between DHT inhibitor use and impairment of erectile function was further solidified:
” Liu et al. (31) performed a systematic review and metaanalysis of 17 randomized controlled trials, including 9,628 men on 5ARIs. Over an average therapy duration of 17.6 months, the relative risk of sexual dysfunction in men taking 5ARIs for BPH was 2.56. This association was not seen in the patients with AGA.
…The greater incidence of erectile dysfunction has even been confirmed with anatomic evaluations. A prospective cohort study of men on a 5ARI for AGA found 48% of them to have a vascular abnormality on penile duplex ultrasound: 32% with arterial insufficiency and 16% with venous leak (29).
Perhaps more alarming are the reports of ongoing sexual dysfunction despite cessation of 5ARI therapy. As Dr. Abdulmaged Traish discussed in his recent Views and Reviews article, postfinasteride syndrome may include persistent erectile dysfunction, delayed orgasm or anorgasmia, loss of penile sensitivity, anhedonia [inability to feel sexual pleasure or any kind of pleasure in daily activities], difficulty concentrating, and loss of muscle mass”
If you’re a man reading this and you’re even thinking about Dutasteride or Finasteride use, just stop.
You’re not doing yourself or your future children any favors.
Cognitive Decline
Dr. Howell was first tuned in to the connection between 5-αR enzyme activity and brain function when he came across a paper showing how sleep-deprived rats exhibit changes in 5-αR within the brain:
“Research by Frau et al. (2017) showed how sleep deprivation-related cognitive and behavioral deficits were exacerbated or negated when 5-α-reductase expression was altered in different brain regions since 5-α-reductases, type 1 and 2, are the rate-limiting catalysts for converting progesterone to 5-α-di-hydro-progesterone [5α-DHP] and testosterone to DHT, both of which are converted downstream into more potent neuro-steroids (allopregnanolone and 3-α-androstanediol).”
(FYI – for the women reading this, Azzouni notes that 5α-DHP “is a major hormone in the circulation of both normal cycling and pregnant women”)
In the same year, a retrospective study in humans sounded a potential alarm:
“We used a matched cohort design and linked administrative data from the province of Ontario, Canada. A total of 99 covariates were measured, and a propensity score was used for matching; 81,162 men who used a 5ARIs were matched to an equal number of men who did not.
New initiation of 5ARI medication was associated with an increased risk of dementia during the first (HR 2.18, 95% CI 2.01–2.35) and second (HR 1.52, 95% CI 1.39–1.67) year, however this risk was nonsignificant among the men with the longest exposure to 5ARIs (HR 1.06, 95% CI 0.98–1.14). There was no difference in the results between types of 5ARIs.
As the strength of the association decreased with increased exposure, the higher risk seen in the initial two years likely represents the presentation and treatment of urinary symptoms which coexist with mild cognitive impairment and eventually progresses to a diagnosis of dementia.”
While the authors stated “the lower risk with increasing use does not suggest a causative relationship”, the evidence since then continued to pile up.
In 2020, yet another review brought up the association between 5-ARIs and cognitive impairment:
“Testosterone protects against age-related cognitive decline and dementia in men. In other words, this result is pharmacokinetic evidence that 5-ARI can cause cognitive impairment and dementia.
In a very recent animal study, 5-ARIs were reported to increase tau phosphorylation and alter dendritic morphology in the hippocampus of male mice, causing cognitive impairment. In this study, the activity of 5-AR was shown to be involved in the production of neurosteroids, and it was concluded that 5-AR plays an important role in neuroprotective effects.
In a population-based retrospective cohort study of male patients 66 years of age or older, 5-ARIs resulted in an increased incidence of self-injury and depression”
Once again, other studies were cited to claim that 5-ARI use is not related to the incidence of dementia… but it won’t be possible to keep up this facade for much longer.
A 2021 cohort study examined nearly 297,000 men who were assigned to two separate groups:
“We identified all men with a hospital inpatient or outpatient clinic diagnosis of BPH [bening prostate hyperplasia], and/or a transurethral resection of the prostate (TURP) and/or at least one prescription for BPH-related medical treatments, defined as alpha-receptor blockers or 5-alpha reductase inhibitors from 1996 to 2016… We excluded men with dementia, mild cognitive impairment, or amnestic syndrome before BPH diagnosis date.”
“The comparison cohort consisted of up to 4 birth-year-matched men from the general population for each BPH patient. Comparison men were not allowed to have a diagnosis of BPH, a TURP, a filled prescription for BPH-related treatment, or a diagnosis of dementia, mild cognitive impairment, or amnestic syndrome recorded before the BPH diagnosis date of the matched patient (index date).”
And here’s what was found:
“The cumulative risk of AD [Alzheimer’s Disease] was consistently higher in the BPH cohort than in comparisons. During 1 to 10 years of follow-up, the cumulative risk of AD was 1·15% (95% CI, 1·11–1·20) in the BPH cohort and 1·00% (95% CI, 0·98 –1·02) in the comparison cohort, corresponding to a 1–10 year risk difference of 0·15%.
Dr. Scott Howell wanted me to emphasize the following finding from the study:
“The adjusted 1-10-year hazard ratios were 1.16 (95% CI: 1.10-1.21) for AD and 1.21 (95% CI:1.17-1.25) for all-cause dementia. From >10 years up to 21 years of follow-up, BPH + 5-alpha reductase inhibitor use remained associated with 10%- 20% increased risk of AD and all-cause dementia.”
One more thing — remember Dave Lee’s article on Pregnenolone, an essential neurosteroid for lowering neuro-inflammation and regulating cognitive function?
Turns out that finasteride might be altering its production in ways even Big Pharma was unable to anticipate:
“In 2014, Caruso et al. examined the plasma and CSF [cerebrospinal fluid] of 7 post-finasteride patients with persistent symptomology and compared their results to 12 healthy volunteers. On average, patients used finasteride for 2 years and discontinued treatment 4.4 years prior to the study… Progesterone was reduced in CSF, its metabolite DHP was reduced in plasma and undetectable in CSF, allopregnanolone was undetectable in both CSF and plasma, and isopregnanolone was raised in plasma. Pregnenolone was raised in both CSF and plasma.“
“In 2017, Melcangi et al. analyzed the plasma and CSF of 14 post-finasteride patients who reported persistent side effects and compared them to a control of 25 healthy subjects. The post-finasteride patients used finasteride for 2.8 years and had discontinued treatment 5.4 years earlier, on average… Of the progesterone metabolites, DHP was lowered in both CSF and plasma while allopregnanolone was undetectable in plasma. The post-finasteride patients also exhibited lower pregnenolone levels in the CSF, but higher pregnenolone levels in plasma.“
Without copying the entire article published by Leo & Longevity here, I want to highlight just one more paragraph which shows why these findings are significant:
“CSF steroid measures are particularly relevant to behavior and cognition because they represent hormones that have either passed the blood-brain-spinal cord barrier or been synthesized in nervous or brain tissue. Progesterone and its metabolite allo-pregnenolone are consistently lowered in former finasteride users with persistent symptomology. This is in line with studies on current finasteride users, while dutasteride totally inhibits allo-pregnenolone synthesis as measured in plasma, even in women”
Are you seeing it yet?
Sodium Conservation
Paraphrasing Azzouni’s paper, Dr. Scott Howell highlights another concern:
“For example, we do not know the effect of inhibiting 5-α-reduction of aldosterone to 5-α-dihydro-aldosterone which is a potent anti-natriuretic metabolite with different physiological effects of aldosterone and its formation in the kidney is increased by restriction of dietary sodium intake, suggesting it has an important physiologic function of conserving sodium.”
We know that sodium regulation is important, as too much sodium in the blood (hypernatremia) or too little (hyponatremia) is bad news:
“Hyponatremia occurs when blood sodium goes below normal levels, which is 135 milliequivalents/liter (mEq/L). When sodium levels in the blood are too low, extra water goes into body cells causing them to swell. This swelling can be especially dangerous for brain cells, resulting in neurological symptoms such as headache, confusion, irritability, seizures or even coma.”
“In hypernatremia, the body contains too little water relative to the amount of sodium, Mount said. This causes sodium levels to become abnormally high in the blood — more than 145 mEq/L — which causes water to move out of body tissues and into the blood in an attempt to equalize the concentration between the two. Water can be lost from brain cells, causing them to shrink, which can be dangerous.”
Who knows what the short-term or long-term consequences could be?
Increased Risk For High-Grade Prostate Cancer
While I’ve already mentioned this undesirable outcome in my most recent article about DHT inhibitors, I wanted to get Dr. Scott Howell’s take on this issue.
A systematic literature review published in 2009 by the American Urological Association listed out guidelines regarding the use of 5-ARIs for prostate cancer chemo prevention:
“For the man who wishes periodic monitoring (opportunistic or organized screening), 5-ARI therapy during a 7-year period reduces the period prevalence of for-cause cancer diagnoses by approximately 25% (relative risk reduction) for an absolute risk reduction of about 1.4%. Although the majority of the Panel judged that the observed higher incidence of high-grade (Gleason score 8 to 10) cancer in the finasteride group is likely due to confounding factors, the increased incidence of high-grade cancer as a result of induction by the drug cannot be excluded with certainty”
Put another way, the possible risks of high-grade prostate cancer from 5-ARI use were judged to be unlikely by the majority of the panel members involved developing evidence-based recommendations from this review.
This observation did not hold for long, as in 2011 the FDA had to put out a safety communication warning physicians of this “unlikely” risk:
“The new safety information is based on FDA’s review of two large, randomized controlled trials––the Prostate Cancer Prevention Trial (PCPT) and the Reduction by Dutasteride of Prostate Cancer Events (REDUCE) trial––which evaluated daily use of finasteride 5 mg versus placebo for 7 years and daily use of dutasteride 0.5 mg versus placebo for 4 years, respectively, for the reduction in the risk of prostate cancer in men at least 50 years of age.
The trials demonstrated an overall reduction in prostate cancer diagnoses with finasteride 5 mg and dutasteride treatment. This overall reduction was due to a decreased incidence of lower risk forms of prostate cancer.
However, both trials showed an increased incidence of high-grade prostate cancer with finasteride and dutasteride treatment”
Fast forward to 2019, and a study of data on nearly 81,000 Veteran Affairs patients collected between 2001 and 2015 who had prostate cancer and used 5-ARIs showed a grim picture:
“Patients treated with 5-ARI were more likely to have Gleason grade 8 or higher (25.2% vs 17.0%; P < .001), clinical stage T3 or higher (4.7% vs 2.9%; P < .001), node-positive (3.0% vs 1.7%; P < .001), and metastatic (6.7% vs 2.9%; P < .001) disease than 5-ARI nonusers. In a multivariable regression, patients who took 5-ARI had higher prostate cancer–specific (subdistribution hazard ratio [SHR], 1.39; 95% CI, 1.27-1.52; P < .001) and all-cause (HR, 1.10; 95% CI, 1.05-1.15; P < .001) mortality.”
You read that right: A 39% increased risk in mortality associated with prostate cancer, and a 10% increased risk in all-cause mortality!
It’s a very sharp contrast to how people tried to link therapeutic testosterone use to worsening heart health (as investigated in The TOT Bible), as researchers pulled insurance records and claim data in an attempt to link a prescription with an outcome (i.e. a secondary data analysis).
The Rise Of Metabolic Disease
Since his pivotal review linking 5-ARI use to sexual dysfunction in 2011, Traish came back in 2020 to suggest 5-ARI use contributes to a host of pathophysiological conditions that have yet to be realized given the lack of studies examining deficiencies in reduced metabolites other than DHT.
Some of the health risks he highlighted include…
Insulin Resistance (IR):
“In humans receiving dutasteride, impaired insulin sensitivity in peripheral organs, including skeletal muscle and/or adipose tissue were recorded. The authors suggested that the adverse changes in IR may, in part, be mediated by impaired glucose disposal, mainly in muscle where 5α-R types 1 is expressed”
Type 2 Diabetes (T2DM):
“Wei et al investigated the incidence of new onset T2DM in men receiving dutasteride or finasteride for long-term treatment of BPH, utilizing the UK Clinical Practice Research Datalink and Taiwanese National Health Insurance Research Database. New onset of T2DM events was recorded during a mean follow-up time of 5.2±3.1 years. There was a modest increased risk of T2DM for dutasteride and finasteride compared with tamsulosin…the risk of developing T2DM was higher for patients receiving dutasteride or finasteride compared with tamsulosin (adjusted hazard ratio [HR]=1.34, 95% confidence interval [CI]=1.17 to 1.54; and 1.49, 1.38 to 1.61, respectively), but the risk for dutasteride and finasteride did not differ (0.90, 0.77 to 1.06) “
Dry Eye Disease:
“Zhang et al and Li et al described the effects of 5α-DHT inhibition by finasteride on ‘lacrimal gland histopathology’ and ‘ocular function’. Finasteride administration effectively induced dry eye in rats by 14 days after administration. Finasteride treated rats had significantly higher fluorescein staining scores and lower aqueous tear quantity and TBUT as compared with control rats. Finasteride significantly diminished tear flow and resulted in severe inflammation of the lacrimal gland. Tear secretion was also significantly reduced in finasteride treated animals compared with control animals on days 14, 21, and 28”
Potential Kidney Disease:
“The physiology of kidney is mediated by ARs [androgen receptors] localized in the cells of most parts of the nephron. Thus, androgen deprivation therapy (ADT) or inhibition of androgen metabolism may affect kidney physiological function. Recently, it was shown that finasteride downregulated AR expression in the cortical region of the kidney. Finasteride treatment resulted in reduction in AR-positive cells in the renal corpuscle (0.06%±0.03%) as compared with untreated animals (0.14%±0.12%). Similarly, the percentage of AR-positive cells in the proximal convoluted tubule of finasteride treated animals also demonstrated marked reductions compared with control animals (0.16%±0.17% vs. 0.69%±0.32%, respectively). “
Nonalcoholic Fatty Liver Disease (NAFLD):
“Dowman et al reported that 5α-Rs types 1 and 2 are highly expressed in human liver and inhibition of these enzymes may elicit adverse metabolic consequences. In the animal model, inhibition of 5α-Rs types 1 and 2 impeded glucocorticoids and androgens metabolism and contributed to the pathogenesis of nonalcoholic fatty liver disease (NAFLD). 5α-R type 1 knockout mice (α-R1KO), which were fed high-fat diet, exhibited increased susceptibility to metabolic dysfunction and liver fibrosis. Furthermore, deficiency in 5α-R type 1 in the animal model predisposed susceptibility to glucose intolerance and hyperinsulinemia “
That’s a whole host of metabolic dysfunctions to deal with!
Another systematic review of 5-ARI use done in 2021 also pointed out effects such as:
- Differential accumulation of body fat
- Obesity, dyslipidemia, hypertension, metabolic syndrome
- Increased intracellular triaglycerol accumulation, inflammation, and impaired fatty acid oxidation.
One final point before I reach the very obvious conclusion…
5-Alpha-Reductase Inhibition Doesn’t Just Impact Humans, But ALL Mammals!
Dr. Scott Howell blew my mind when he showed me another pivotal paper examining the consequences of 5-ARI use in mammalian vertebrates on androgen-dependent organs.
Published in 2020, here are just some of the findings highlighted:
- Atrophy of androgen-dependent organs: Prostate, epididymis, seminal vesicles, corpus cavernosum.
- Decreased proliferation of sex organ cells, presence of fibrosis in the corpus cavernosum, increased apoptosis of prostate cells, alteration in tissue morphology.
- Decreased erectile function, penile atrophy, decreased neuronal nitric oxide synthase, fibrosis of penile tissue, and long-term exposure causing permanent damage.
- Impaired bone development, turn over and retention.
- Reduction in brain allopregnenolone levels leading to anxiety since progesterone must be reduced to form this neuroprotective metabolite.
- Reduction in brain allopregnenolone levels leading to seizures.
- Alteration in aggression by varying reduction of testosterone into androstenediol in the brain.
- Liver-steatosis, increased visceral body fat, and insulin resistance.
There are numerous researchers (here, here, here, and here) who have been trying to warn society of the consequences of long-term 5α-reductase inhibition.
The world may not listen, but hopefully you can.
CONCLUSION: Are You REALLY “Just” Blocking DHT Production!?
(Source)
When 5-α-reductase blockages occur long-term through the use of inhibitors, it causes a unique form of androgen deficiency characterized by the loss of DHT and, more importantly, deficiencies in other potent steroid hormone metabolites that the 5-α-reductase enzyme catalyzes.
So when your doctor prescribes Finasteride or Dutasteride to prevent hair loss, you are NOT just blocking DHT:
You are directly interfering with numerous biological systems in your body involving +15-20 different steroid hormones.
There are a lot of potential downstream consequences that have been largely ignored by the pharmaceutical companies making them, either out of ignorance or intention to mislead health regulators and the public at large.
With Big Pharma’s track record, I’ll let you be the judge.
PART 2: Estrogen Inhibiting Drugs

As I did with the DHT inhibitors, there’s some introductory reading necessary to understand what I’m going to be talking about.
So please read my articles on the dangers of estrogen-inhibiting drugs and why it’s leading to a “killing” of competitive bodybuilders.
And when you’re finished, much of what I’m going to briefly list off here is featured in this presentation Dr. Scott Howell gave to me last year:
Even back in 2006, we knew the following:
- Brain — Aromatase deficiency (the enzyme converting testosterone to estrogen) and knock out studies show that estradiol is neuroprotective and essential to the integrity and survival of dopaminergic neurons, mood stabilization, and normal sexual behavior in males
- Immunity — Estrogen is also essential and vitally protective on the immune and cardiovascular systems
- Metabolism — Men with true aromatase deficiency have insulin resistance and impaired carbohydrate metabolism, which is replicated in aromatase knock out models and leads to metabolic syndrome.
- Bone strength — Men with aromatase deficiency experience increase bone remodeling, unfused epiphyses, and reduced bone mineral density, thus the current body of evidence supports the essential role of estrogen in bone growth and homeostasis in men.
We even see cognitive decline in WOMEN who have their estrogen levels artificially tampered with:
“Surgical menopause also leads to harmful effects on cognition. The Mayo Clinic study demonstrated a doubled long-term risk of cognitive impairment or dementia in women who underwent oophorectomy before menopause (124). The risk of cognitive impairment and dementia increased with younger age at the time of oophorectomy. This risk was eliminated in women who received HRT after surgery until 50 years of age, but those who received HRT and stopped before age 50 years had an elevated risk of cognitive impairment and dementia that increased with younger age of stopping this therapy”
That was just one of many conclusions reached by the authors of this paper, who are worried that estrogen deprivation may lead to age acceleration:
“Estrogen deprivation in healthy women younger than 50 years undergoing bilateral oophorectomy has been shown to accelerate the development of diseases related to aging, including coronary artery disease, cardiac arrhythmias, stroke, dementia, and osteoporosis, raising concern that even less dramatic modulation of estrogen homeostasis may adversely affect health outcomes.”
(HIGHLY recommend you read the entire paper if you want to know how and why estrogen is important in virtually every human biological system)
The Connection Between Estrogen And Heart Health
This is the one benefit I want to focus on more than any other, as it singularly shows how estrogen-inhibiting drugs such as aromatase inhibitors (AIs) and selective estrogen receptor modulators (SERMs) are killing people at a young age.
So let me start by highlighting this important part of Dr. Scott Howell’s presentation:
“E2 [estrogen, aka estradiol] binding to ERβ [estrogen receptor beta] and ERα [estrogen receptor alpha] to cardiomyocytes is essential to maintain cardiac health. In the absence of E2 binding, the adaptive hypertrophy from androgens is magnified and begins the progression to pathologic remodeling. Estrogen receptors are also expressed in cardiac endothelial cells and smooth muscle cells to carry out a broad range of benefits to the heart.
E2-activated membrane ERβ signaling prevents cardiac hypertrophy through posttranslational modification of the NFAT (nuclear factor of activated T cells) family of transcription factors that sequester these proteins in the cytoplasm of cardiomyocytes.
Estradiol-ER binding in cardiomyocytes also activates kinase signaling pathways that attenuate pathologic cardiac hypertrophy.
Membrane ERβ binding of estradiol also suppresses cardiac fibrosis through signaling to SMAD sequestration in the cytoplasm of cardiac fibroblasts “
This is directly linked to the four main reasons that bodybuilders are dropping dead:
- Cardiac pathology caused by chronic cardiac strain via pressure or volume overload through uncontrolled hypertension through systematic activation of the renin-angiotensin-aldosterone system, elevated Ang II and 20-HETE.
- Residual cardiac strain by carrying 50-100lbs more than genetic weight and meeting the tissue oxygenation demands of this unnatural amount of tissue on a daily basis
- Chronic aromatase inhibition that prevents estrogen to counter the pathologic hypertrophy and collagen remodeling by binding to beta and alpha estrogen receptors, respectively.
- Resistance training exacerbation of androgen-induced hypertrophy.
Add in extreme resistance training, supraphysiological doses of testosterone, and anabolic steroids, and you have a very nasty case of cardiomegaly (an enlarged heart)… this pathological remodeling of the heart does NOT end well.
The most obvious and tragic example of this happening is the late and great John Meadows, one of the most well-known bodybuilding competitors and coaches in the fitness industry.
In 2020, his family reported that Meadows had suffered a heart attack and needed surgery to remove blood clots from his coronary arteries.
Even though this was a result of a rare blood disorder he was diagnosed with in 2005, many commenters on bodybuilding forums around 2016 (here, here, and here) noted his use of Novaldex (a SERM) during his cycles:
“His view, which does talk to the science, is that estradiol is anabolic so reducing it dramatically with a Arimidex/ Letro or Aromasin ( AÍ) is counterproductive to growth. Of course you don’t want this estradiol to bind to receptor sites in say your nipples (causing gyno) therefore using a SERM like Nolvadex resolves this by binding to these receptor sites protecting you from the sides. John only uses AI’s close to [competing] to get rid of the water retention and assist with fat reduction.”
He tragically passed away in the late summer of 2021, with the cause of his death being unknown.
But given how SERMs can increase one’s risk of thrombosis, it’s not unreasonable to assume it was a contributor.
John was truly one of the best human beings I have ever met in my entire life — a humble, down-to-earth, amazing man, husband, and father.
And it is truly tragic to see how rampant estrogen inhibition has taken the lives of so many competitive bodybuilders over the past 20 years.
While AIs and SERMs were used prolifically from the mid-2000s within the bodybuilding industry, around 2013-2015 was when myself and many others discovered the dangers of estrogen inhibition.
As I’ve said before:
Testosterone MUST be converted into the pleiotropic hormone estradiol “E2” (via the aromatase enzyme) to manifest its numerous therapeutic benefits to biological systems!
Many bodybuilders are actively shortening their lifespan via the use of non-aromatizing anabolic drugs and tearing up their vascular pathways… I can guarantee almost every one of them who’s no longer with us died due to the micro-fissures created in their vascular networks.
This whole idea of “maximize testosterone and minimize estrogen” at all costs HAS TO STOP!
Where many of these bodybuilders fall astray is when they get their blood work done a few weeks after getting off a cycle and then assume they’re in great health… forgetting that’s NOT what their bloods look like 99% of the year while running gear.
Dante Trudel had a great Instagram post about this a while back:

How To Reduce The Harm Done By DHT Inhibitors And Estrogen Inhibitors To Your Health

So what’s the next step for people reading this article?
First, make sure you get caught up to speed with Dr. Howell and his extensive treasure chest of wisdom.
Watch his podcast series on therapeutic testosterone (Part 1 and Part 2) along with his overall philosophy on hormone optimization (Part 1 and Part 2)
Second, please reach out to Dr. Howell for a consult if you have been harmed by DHT inhibitors or estrogen inhibitors, or simply need personalized guidance with hormonal health.
He is the world’s leading expert on “harm reduction” for men and women looking to optimize their health through pharmaceutical means.
You can reach him at [email protected]
Dr. Howell and I plan on collaborating within the next year with super advanced courses.
He and I will be also doing some upcoming podcasts and livestreams with Victor Black among other online influencers focused on helping humanity move into the Golden Age.
Speaking of courses, my Testosterone Optimization Therapy Decoded Course debuts soon.

As always…
Raise Your Vibration To Optimize Your Love Creation!
PS – If you want to master this subject on a much deeper and esoteric level to improve the quality and quantity of your life, sign up for The Fully Optimized Health Private Membership Group.
In addition to full-on access to Daniel Kelly and I, you’ll be able to reach new levels of physical and well-being with a group of high-conscious, like-minded men and women.
You’ll also get access to our best-selling books and webinars for free, state-of-the-art testosterone optimization, cutting-edge research on peptides and supplements, interviews with spiritual masters, and our “black book” Rolodex of the world’s best hormonal health physicians.